
Race-Based Disparities in Insurance Coverage Among Cancer Survivors
Marshall, J.
Author correspondence: info@stem4humanrights.com
Cite this article: Marshall, J. (2023). Race-Based Disparities in Insurance Coverage Among Cancer Survivors. Diverse Perspectives on Wellness, 1(2), 1-7.
Abstract
Although cancer negatively impacts almost every family across generations, racial minorities’ experiences with cancer diagnosis, treatment, and insurance coverage are arguably unique. This article assesses the extent to which demographic characteristics predict coverage denial for cancer treatment, and results reveal that among those with cancer, racial minorities are at least twice as likely to be denied coverage for treatment. However, senior citizens, a large majority of whom are supported by Medicare’s clear policies on cancer treatment have lower odds of being denied coverage, suggesting that racial minorities who rely on private insurers may benefit from additional clarity regarding coverage-related benefits.
Keywords: health insurance, coverage denial, cancer
Introduction
Cancer is the second leading cause of death in the United States, and while it negatively impacts almost every family across generations, the way that racial minorities experience cancer is arguably unique (Lent et al., 2022). Cultural hypermasculinity can, in many cases, create a tendency for cancer-related stigma, disregarded symptoms and diagnosis concealment, and prior poor health care experiences may have an adverse impact on care-seeking behaviors. These common hallmarks of the minority cancer care experience are often reflected via delayed screenings, missed or reluctantly attended doctor appointments, friction in the patient-provider relationship and lost opportunities for emotional and financial support. When compounded by financial hurdles from insurance-related barriers, the weight of issues related to care, costs and coverage may compromise treatment decisions and have a lasting impact on patients’ emotional, psychological and overall well-being.
Barriers to Clinical Trials
While most cancer treatment is accessed in traditional health care settings, clinical trials offer research-based interventions where new drugs and/or novel treatment strategies have been credited with both improved survival rates and positive behavioral changes for participants. While there is widespread belief among oncologists that clinical trials offer a better opportunity for effective cancer treatment, access to the benefits of clinical trial care remain elusive for many outside of mainstream demographic groups, including those of minority race (Peppercorn et al., 2004). Admissions criteria favors low morbidity and early-stage participants which disadvantages minorities due to a higher tendency for chronic disease and late-stage cancer diagnoses, and limited clarity regarding clinical trial availability, admissions requirements, mistrust of research due to historical violations, and logistical dilemmas (e.g., taking off work, arranging childcare, traveling to cancer centers) have persisted for decades as serious impediments to access. Inequitable access also negatively impacts researchers who hope to achieve generalizable results. However, given the high costs of clinical trials, the pre-authorization process that insured cancer patients must undergo to seek approved coverage situates insurance companies as gatekeepers of treatment, and adequate health coverage as a key facilitator of access. Multiple studies revealed that 81% of denials were due to inadequate insurance which did not cover trial participation (Charlot et al., 2022; Klamerus et al., 2010; Mackay et al., 2017). Unlike Medicare which has a clear policy of covering specific cancer treatments and clinical trial access depending on the plan type (e.g., Part A, Part B, etc.), coverage decisions for some private payers are considered on a case-by-case basis, making public knowledge of health insurance benefits and decision-making processes critical to navigating admissions hurdles and avoiding high out-of-pocket costs.
Cost-related Barriers
According to one study, 50% of cancer patients experience financial hardship from the impact of cancer care costs (Panzone et al., 2022). Even with adequate insurance coverage, cancer treatment can prove costly, and when combined with prospective wage losses, has the potential to financially devastate low and middle-income households. 42% of cancer survivors report cancer sickness as a barrier to workplace productivity, and 63% report adverse salary impacts due to a declined promotion, taking extended time off or scaling back to work part-time (Nekhlyudov et al., 2016). Although an impact from financing insured care is unavoidable to some degree and making the incorrect Medicare plan choice and not having the appropriate benefits (e.g., lack of a clinical trial, lack of an out-of-state benefit, etc.) to accommodate one’s individual circumstances can restrict covered access to preferred modes of treatment (Nipp et al., 2015). Lack of a clinical trial benefit greatly reduces odds of clinical trial coverage, and lack of an out-of-state benefit often leads to insurance denial for cancer patients near state borders when higher quality or more affordable care is just across the state line. Unfortunately, 45% of Americans report inadequate health insurance coverage (Panzone et al., 2022). Considering that the bulk of this uninsured population are racial minorities who are also negatively impacted by wealth inequality, racial disparities in cancer treatment, cancer treatment quality and cancer survivorship are likely to persist without large-scale efforts to streamline access to adequate health coverage.
Racial Disparities in Insurance Coverage and Cancer Treatment
Racial identity often frames the cancer care insurance conversation since minority status consistently predicts underinsurance, limited access and lower quality of care, leading to Blacks having the highest death rates across a variety of cancer types. 17.8% of Hispanics and 15.0% of Blacks report receiving no cancer treatment, and when compared to just 6.0% of Whites (P <.001), demonstrates the vast differences in cancer care access for minorities (Panzone et al., 2022). Cervical cancer rates remain high among Black and Hispanic women even though vaccinations and early screenings are widely available, and Black patients have lower rates of timely surgery and more clinically relevant delays for chemotherapy despite the critical relationship between the receipt of timely care and survival (Green et al., 2018). Given the need for adequate insurance to facilitate cancer care treatment, this analysis seeks to both identify race, gender and age-related disparities in health insurance denials, clarify which demographic characteristics are associated with limited access to cancer care coverage and discuss opportunities for improved access that exist within the context of insurance approval processes, clinical care and community-wide approaches.
Methods
The Behavioral Risk Factor Surveillance System (BRFSS) is an annual health survey offered by individual states and territories on behalf of the U.S. Centers for Disease Control. Annual data are collected using random digit dialing to recruit participants through cell phones and landlines and assess population health and health-related behaviors. Data from the cancer survivorship module were obtained from the 2020 BRFSS survey to produce estimates for cancer survivors who were denied insurance coverage. Responses to the question “Were you ever denied health insurance or life insurance coverage because of your cancer?” were coded as a dichotomous (e.g., yes/no) dependent variable, and estimates were produced by demographic sub-group with race/ethnicity serving as the main independent variable. Race/ethnicity counts were based on an analytical approach that includes participants with Hispanic ethnicity and non-Hispanic participants with single-race membership. While counting participants with multiple race membership based on preferred race can sometimes help avoid excluding Native Hawaiian and Other Pacific Islanders whose members tend to identify as two or more races, in this instance, neither approach yielded a large enough count of Native Hawaiian and Other Pacific Islanders to produce reliable estimates. Logistic regression analyses, proportions and odds ratios were calculated to determine the extent to which race, sex and age would predict coverage denial due to cancer, variables were weighted using standard BRFSS weights to adjust for gender by age group, race/ethnicity, education, marital status, tenure, gender by race/ethnicity, age group by race/ethnicity and phone ownership, and all analyses were conducted using R version 4.2.0.
Results
The logistic regression model revealed that minority race (β = 0.72, p < 0.001), female sex membership (β = 0.26, p = 0.001), and age groups 40-64 (β = -0.17, p < 0.001) and 65 and older (β = -1.01, p < 0.001) each had a statistically significant effect on being denied health or life insurance due to cancer. Given the results of the logistic regression, the minority race variable was further disaggregated to assess the proportion of insurance denials for each race and ethnic group. These proportions, along with those for sex and age are available in Figure 1.
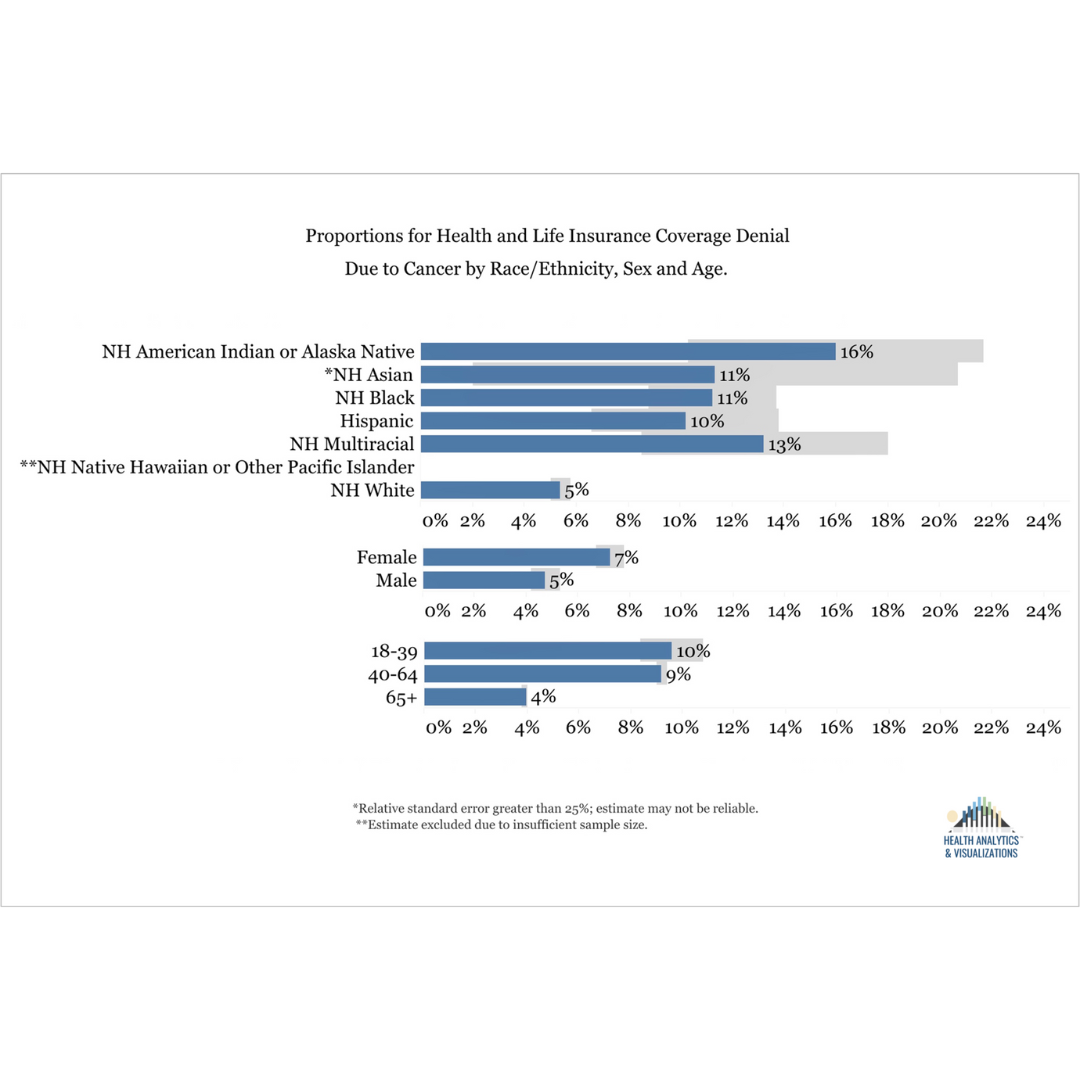
For American Indians or Alaska Native cancer survivors, 16.0% (95% CI: 10.3, 21.7) reported being denied health or life insurance compared to just 5.4% (95% CI: 5.0, 5.8) for Whites. For female participants, 7.3% (95% CI: 6.7, 7.8) received denials compared to 4.7% (95% CI: 4.2, 5.3) for males. Across all demographic sub-groups, denials were lowest for older adults ages 65 and older at just 3.9% (95% CI: 3.8, 4.0).
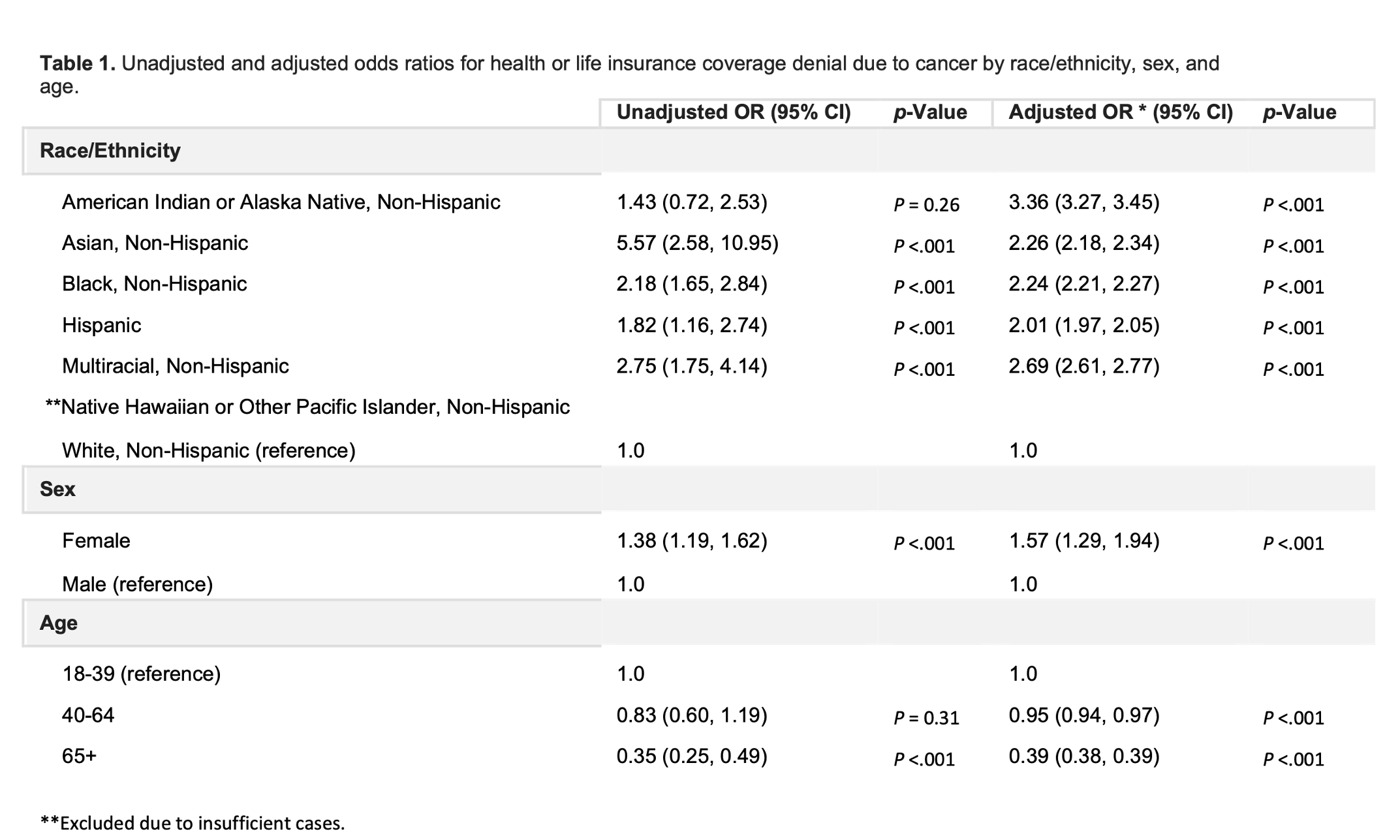
As shown in Table 1, each minority race group had at least twice the odds of being denied health or life insurance due to cancer, including American Indian or Alaska Natives who had three times the odds (adj. OR = 3.36, P < .001). Insurance denial odds for females were higher when compared to males with a statistically significant difference (adj. OR = 1.38, P < .001), and adults ages 65-plus, when compared to younger adults ages 18-39 had lower odds of being denied insurance (adj. OR = 0.39, P < .001).
Minority race as a significant predictor of being denied health or life insurance may be at least partially attributable to each group’s high risk of comorbidity given its impact on coverage decisions. Significantly higher insurance denials among female cancer survivors reflect the inequities of gender bias in health care which restrict both access and quality of care. Women are also more likely to undergo genetic testing which might expose them to potential insurance denial due to genetic discrimination, even though the Genetic Information Nondiscrimination Act (GINA) makes the use of genetic information in eligibility and coverage decisions illegal (Otlowski, 2012). Given that case-by-case decision making facilitates an opportunity to introduce both systemic and interpersonal biases that may limit access to cancer care for race and gender minority groups, adapting these decision-making processes using an equity-based framework and clarifying new processes may reduce rejection odds among minorities. For example, while the data also indicate an inverse relationship between age and odds of insurance denial due to cancer, this relationship is most likely attributable to high Medicare enrollment among seniors and Medicare’s clear policy of covering chemotherapy and routine costs for clinical trials, which further suggests that private payers who adopt clear policies with consistent implementation may positively impact cancer coverage disparities. Furthermore, although this article does not address cancer care in detail, more work is needed to reduce time delays for chemotherapy, surgery, and other cancer treatment modalities among minorities, especially given that reduced time delays are a metric of quality care. Low quality care experiences undoubtedly contribute to tension between some minorities and health care providers. However, many health care systems possess the resources to mitigate these burdens and should consider research-based antiracist interventions for equitable treatment, especially in a context as critical as cancer care (Aina et al., 2019). Also, more research is needed to determine the extent to which cultural views on socially appropriate sickness work against care-seeking behaviors and motivate diagnosis concealment. Minority communities might also consider whether in addition to trusted treatment providers, there are safe spaces for its sick members to seek support while avoiding the added stressors of shame and stigma, and individual patients hoping to optimize their own engagement in cancer care should work to prioritize understanding how different insurance benefits might impact their current and future health care.
Limitations
Analyses were based on data from the year 2020 during which the COVID-19 pandemic was in its early stages. The COVID-19 pandemic greatly impacted data gathering operations for many social and health surveys and may have affected response rates and distribution of participant characteristics. The survey question upon which analyses are based asks participants about health or life insurance; however, a decision was made to narrow the article’s focus to health insurance while acknowledging the critical need for more discussion regarding disparities in life insurance coverage decisions. Also, these responses were self-reported and thus could not be validated. Finally, the survey question upon which analyses are based asks cancer survivors about a past and potentially traumatic event, making recall bias a potential limitation.
References
Charlot, M., Stein, J.N., Damone, E., Wood, I., Forster, M., Baker, S., Emerson, M., Samuel-Ryals, C., Yongue, C., Eng, E., Manning, M., Deal, A. & Cykert, S. (2022). Effect of an antiracism intervention on racial disparities in time to lung cancer surgery. Journal of Clinical Oncology, 40(16), 1755-1762.
Green, A.K., Aviki, E.M., Matsoukas, K., Patil, S., Korenstein, D. & Blinder, V. (2018). Racial disparities in chemotherapy administration for early-stage breast cancer: A systematic review and meta-analysis. Breast Cancer Research and Treatment, 172, 247-263.
Klamerus, J.F., Bruinooge, S.S., Ye, X., Klamerus, M.L., Damron, D., Lansey, D., Lowery, J.C., Diaz, L.A., Ford, J.G., Kanarek, N. & Rudin, C.M. (2010). The Impact of insurance on access to cancer clinical trials at a comprehensive cancer center. Clinical Cancer Research, 16(24), 5997–6003.
Lent, A.B., Garrido, C.O., Baird, E.H., Viela, R. & Harris, R.B. (2022). Racial/ethnic disparities in health and life insurance denial due to cancer among cancer survivors. International Journal of Environmental Research and Public Health, 19(4), 2166.
Mackay, C.B., Antonelli, K.R., Bruinooge, S.S., Saint Onge, J.M. & Ellis, S.D. (2017). Insurance denials for cancer clinical trial participation after the Affordable Care Act mandate. Cancer, 123(15), 2893-2900.
Nekhlyudov, L., Walker, R., Ziebell, R., Rabin, B., Nutt, S. & Chubak, J. (2016). Cancer survivors’ experiences with insurance, finances, and employment: Results from a multisite study. Journal of Cancer Survivorship, 10, 1104-1111.
Nipp, R.D., Powell, E., Chabner, B. & Moy, B. (2015). Recognizing the financial burden of cancer patients in clinical trials. The Oncologist, 20(6), 572-575.
Otlowski, M., Taylor, S. & Bombard, Y. (2012). Genetic discrimination: International perspectives. Annual Review of Genomics and Human Genetics, 13, 433-454.
Panzone, J., Welch, C., Morgans, A., Bhanvadia, S.K., Mossanen, M., Shenhav-Goldberg, R., Chandrasekar, T., Pinkhasov, R., Shapiro, O., Jacob, J.M., Basnet, A., Bratslavsky, G. & Goldberg, H. (2022). Association of race with cancer-related financial toxicity. JCO Oncology Practice, 18(2), e271-e283.
Peppercorn, J.M., Weeks, J.C., Cook, E.F. & Joffe, S. (2004). Comparison of outcomes in cancer patients treated within and outside clinical trials: Conceptual framework and structured review. The Lancet, 363(9405), 263-270.
Acknowledgements
This research was supported by Health Analytics & Visualizations.
Rights and Permissions
Health Analytics & Visualizations supports the redistribution of its journal articles and content while also protecting its intellectual property from infringement. To request permission to republish our articles or content, email the Editor-in-Chief at info@stem4humanrights.com.
Conflict of Interest
The authors declare no conflict of interest or financial incentive. The author’s relationships with the stakeholders and subject matter did not lead to unreasonable bias or compromise the objectivity of the research.
All Articles
Barriers and Facilitators to Racial Equity in K-12 Education: An Integrative Review
Race-Based Disparities in Insurance Coverage Among Cancer Survivors
Social Dynamic Response Theory
The Global Impact of the COVID-19 Pandemic on Maternal Mortality
Reducing the Body Count During the Next Pandemic
Math Anxiety Interventions to Address the STEM Gender Gap for Girls